

We said in the beginning that the United States has some of the highest costs and unequal access, with only average health outcomes. The figure below (which figure???) presents data from OECD (The Organization for Economic Co-operation and Development). OECD collects data on economics and policy for the 34 member nations. Health is one of the many topic areas. The figure below presents results from the 2011 report of health indicators.
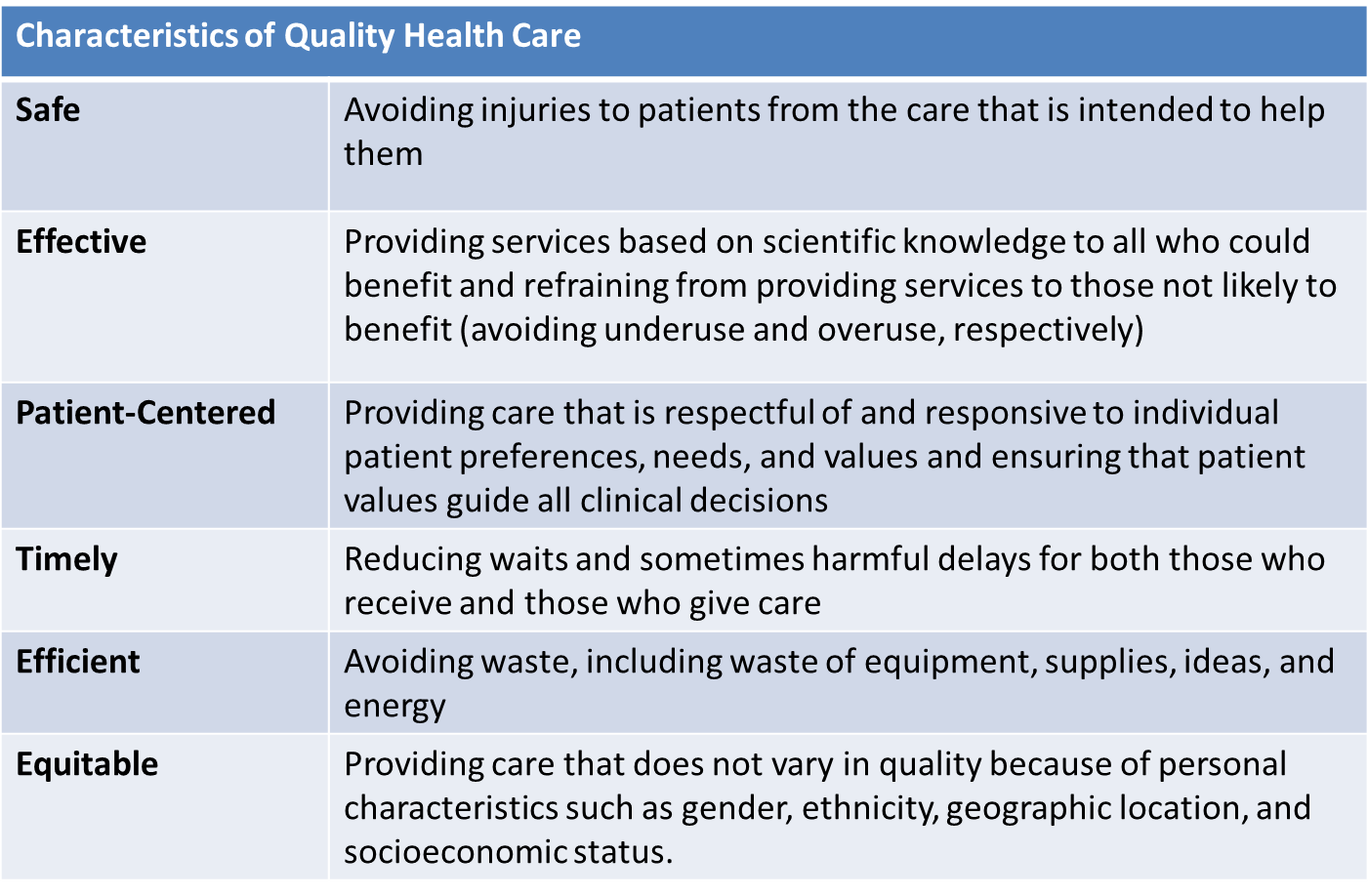
The Definition of Quality
"Quality is the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge."
Institute of Medicine , McGlynn, 1997, as quoted in Shi & Singh, 2008
According to Shi and Singh (2013), both micro- and macro-perspectives determine quality. For example, some micro quality indicators might be small area variations, medical errors, patient satisfaction, quality of life, and health outcomes. Macro quality indicators would be cost, access, and population health.
|
Micro Quality Indicators |
Macro Quality Indicators |
|
|
Structure, process, and outcomes in determining quality are closely linked, as shown below. Here are some simple definitions:

Ideally these are linked horizontally. The structural characteristics impact or inform the processes. The processes then impact or inform the outcomes.
In quality improvement it is said that you can't improve what you can't measure. Is that true? Maybe. Or maybe you can't track improvement. What if your efforts to make things better really makes them worse?
More Process and Outcome Measures
What do or should we care about the most if we take the patient-centered perspective? Outcomes. We want to know how things turn out for the patient. What do we tend to measure? Processes. Why? Because that is what we control (can improve) and it is what we can most easily measure. We hope that what we do truly makes a difference in the patient's outcome.
Think about this example. We want to decrease mortality from cardiovascular disease in a cohort of patients being followed at a medical practice. That can be hard to measure. Unless your cohort is pretty old you may have to wait a long time to see the outcome, or you may not even be able to. People move, change insurance, or change primary care.
Then add another layer. How much of health is attributable to medical care? We saw that race/ethnicity, income and education make a difference. Can a PMD change those patient characteristics? From the biophysical perspective, what do we believe impacts cardiovascular disease: genetics, diet, diabetes, age (although we can age-adjust the results), obesity, smoking, the list goes on.
What might the practice decide to measure? Cholesterol levels of patients - patient outcome. Again though, how much does the doctor impact that? You are looking at an absolute measure. What if a patient came in with cholesterol of 350 (high) and working with the PMD got it down to 200 (still elevated). The PMD gets no credit.
What might get measured, especially in a practice with an electronic record, are: what percent of patients had cholesterol checked (process) what percent of patients with elevated cholesterol are on an appropriate medication regimen; and what percent of patients with an elevated cholesterol had documentation of counseling regarding diet and exercise.
Do these process measures actually matter to what happens to the patient in term of cardiovascular mortality? Answer: unclear.

 |
Click on the cards below. For each item drag the card from the bottom to the correct category (process, structure, or outcome). |
|
This content requires JavaScript enabled.
|
|
