



Pharmaceutical Interventions
Vaccination
The World Health Organization has developed a global surveillance program in which virus strains are collected by national flu centers around the world and samples of interest are sent to WHO's advanced laboratories for further assessment.
Every year, WHO suggests three virus strains (2 influenza A and 1 influenza B) to be included in each country's upcoming flu vaccine (FLU, 2011). Selection is based on circulation and ability to cause mass illness in the coming flu season. The chosen strains used to create the vaccine will provide protection against strains that are the same or related.
As indicated above, WHO only provides a recommendation for the upcoming flu vaccine and each country makes the final decision for their population. In the United States, the Food and Drug Administration (FDA) makes the final decision (FLU, 2011). The FDA has chosen A/California/7/2009 (H1N1)-like virus, A/Perth/16/2009 (H3N2)-like virus, and B/Brisbane/60/2008-like virus to be included in the 2011-2012 flu vaccine (CDC, 2011).
Two types of vaccines are manufactured for influenza:
- vaccines containing inactivated ("killed") influenza virus
- vaccines containing attenuated virus
Inactivated vaccine—consists of dead viruses that are given through injection. The three types of flu shots available are regular (>6 mo. of age), Fluzone High-Dose (>65 yrs. old) and intradermal (18-64 yrs. old) (CDC, 2011).
- The amount of antigen in Fluzone High-Dose vaccines is fourfold that of regular flu shots to increase the amount of antibodies for a more robust immune system (CDC, 2011).
- The intradermal flu vaccine has fewer antigens and is injected into the skin and not the muscle.
- Side effects that may result from a flu shot include: soreness, redness, swelling or toughness and itching (only from intradermal vaccine) of the punctured area, and low grade fever and aches (CDC, 2011).
Attenuated vaccine—also known as live attenuated influenza vaccine (LAIV), is available as a nasal-spray (FluMist). As indicated by its name, the virus within the vaccine is weakened and will not cause the recipient to get the flu. Individuals under the age of 2 and over 49, pregnant, have a chronic medical condition, a weakened immune system or take medications that weaken their immune system should not get the vaccine (CDC, 2011).
Unless there is a contraindication, everyone 6 months of age or older should get vaccinated. However, vaccination is particularly important in certain groups. The following table from the CDC provides a list of those who should be most strongly encouraged to get vaccinated and also provides a list of those in whom vaccination is contraindicated.
Who Should Get Vaccinated
- Pregnant women
- Children < 5, especially those between 6 months and 2 years of age
- Individuals > 50
- Individuals who are immunosuppressed or who have chronic medical conditions, including morbid obesity
- Individuals living in long-term care facilities
- Healthcare workers
- Individuals who are in contact with those who are at high-risk for complications or around children < 6 months old
Who Should Not Get Vaccinated
- Individuals allergic to eggs
- Individuals who have had a severe reaction to the Influenza vaccine
- Children < 6 months
- Individuals with moderate-to-severe illness with a fever
- Individuals who developed Guillain-Barre Syndrome after receiving the influenza vaccine
Prioritization of Vaccine
In the past, emphasis has been placed on vaccinating individuals in high risk categories and healthcare providers during vaccine shortages first. In addition, sub-prioritizing is conducted at the discretion of state and local health officials and healthcare providers (CDC, 2011).
In the state of Massachusetts, high risk categories and their order of priority are (MA Department of Public Health, 2004):
- All children aged 6-23 months
- Adults aged > 65 years
- Persons aged 2-64 years with underlying chronic medical conditions
- All women who will be pregnant during the influenza season
- Residents of nursing homes and long-term care facilities
- Children aged 6 month-18 years on chronic aspirin therapy
- Health-care workers involved in direct patient care
- Out-of-home caregivers and household contacts of children aged <6 months
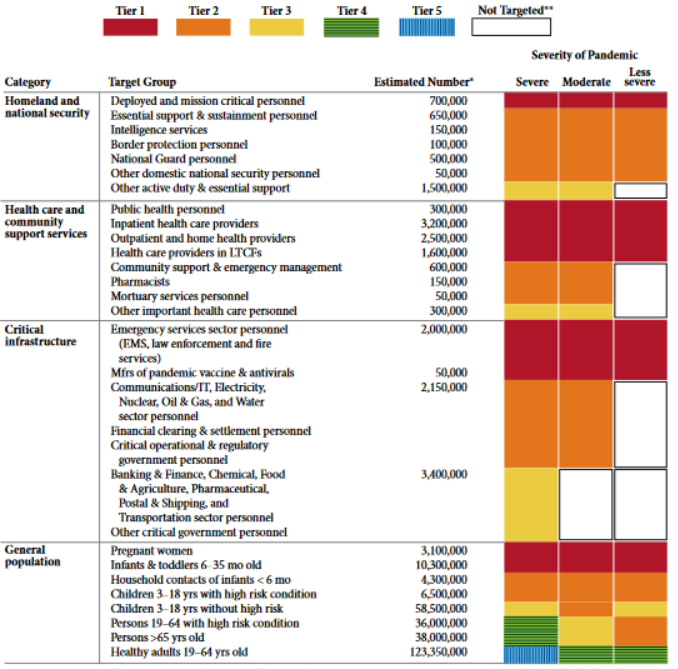
In the case of a pandemic, prioritization is illustrated in the figure below from the CDC.
Title: Vaccination target groups, estimated populations, and tiers for severe, moderate and less severe pandemics as defined by the Pandemic Severity Index (PSI).
Persons in occupational groups not specifically targeted for vaccination in Moderate and Less Severe pandemics are targeted according to their age and health status in the general population.
 ; .
; .
Source: http://www.flu.gov/images/reports/pi_vaccine_allocation_guidance.pdf
However, new information suggests that traditional prioritization of the elderly over healthy young adults and children during shortages of vaccine and pandemics should be reconsidered. Past research has revealed that children are high-transmitter groups (as cited in Miller et. al, 2008). This is most likely due to poor hygienic habits and minimal to no exercising of social distance when infected. Research findings have also suggested using children to create herd immunity as it is more effective to immunize a small group of children to protect the elderly than it is to immunize a very large group of the elderly (as cited in Miller et al, 2008; Radonovich, Bender, & Small, 2007). Consequently, because annual epidemics tend to hit school children first, there may be a rationale for vaccinating them first, rather than last. Overall, there is a greater potential to control the spread of influenza by vaccinating healthy young adults and children before the elderly. This is further illustrated by the following facts (Miller et. al, 2008; as cited in Miller et. al, 2008; Randonvich et. al, 2007):
- Higher mortality rate in younger adults during pandemic seasons and a higher mortality rate in the elderly during interpandemic seasons
- Lower vaccine efficacy in the elderly compared to young adults by 25%-50%
- Lower mortality rate in the elderly during pandemics possibly due to "recycling of influenza viral antigens over time"
- "Immunizing 70% of schoolchildren may protect the entire community"
Flu Vaccine Distribution in Massachusetts
In the state of Massachusetts, it is estimated that there will be a shortage of flu vaccine during the 2011-2012 flu season as a result of billion dollar budget cuts. Consequently, in the coming year state-supplied vaccines will be prioritized for children who are 6 months —18 years of age within identified cohorts and uninsured or underinsured adults who are at high-risk for complications if infected with the influenza virus (MASS, 2011).
Massachusetts recommends (MASS, 2011):
- Vaccinations take place as soon as vaccines become available
- Vaccinating as long as influenza virus is circulating within the community
- Providing end of the season flu shots to children < 9 years of age with their second dose of vaccine if only vaccinated once and travelers going to the Southern Hemisphere who did not get a flu shot at the beginning of the season
All licensed healthcare facilities are required to offer their employees free flu vaccinations according to state regulations within 105 CMR (MASS, 2011). To ensure yearly provision of state-supplied flu vaccine, all healthcare workers are required to report state-supplied vaccine usage to MDPH by the specified deadline (MASS, 2011).
Monitoring Vaccine Safety
Through the Vaccine Adverse Event Report System (VAERS) and the Vaccine Safety Datalink (VSD) Project, the CDC, FDA, and their partners are able to monitor the safety of the current flu vaccine by identifying adverse events and health complications that take place following vaccination (CDC, 2011). The data provided is also a means for: monitoring pattern changes in known adverse events, assessing the safety of groups that are at high-risk for complications, identifying individuals with a greater risk for certain adverse events, and assessing the safety and effectiveness of vaccine lots [insert rollover—batch of vaccine] (CDC, 2011).
Antiviral drugs
These drugs are designed to treat infection and any associated complications of individuals infected with the influenza virus or serve as a form of prevention for non-infected individuals who are allergic to eggs, have developed Guillain-Barre Syndrome from exposure to the influenza vaccine or have a negative immune response to the vaccine. They consist of Amantadine (Flumadine), Rimantadine, Zanamivir (Relenza), and Oseltamivir (Tamiflu).
- Amantadine & Rimantadine—are both adamantanes that were very effective against Influenza A. Recent experience with H3N2 and H1N1 strains has demonstrated the rapid development of drug resistance. Consquently, use of these agents for prophylaxis or treatment of routine cases is not recommended (CDC, 2011).
- Zanamivir & Oseltamivir—are both neuraminidase inhibitors that are effective against Influenza A and B. We are currently limited to these antivirals. Cases of resistance to these antivirals have taken place in both Influenza A and B strains in past years (CDC, 2011). However, the percentage of cases was low and the currently circulating strains are still susceptible to antivirals (CDC, 2011). CDC maintains an ongoing surveillance of resistant cases.