Providers and Hospitals
How They Are Paid
|
|
|
Analogy: Ways to Pay for Food |
|
|
Paying Providers |
|
|
Paying Hospitals |
|
|
Conclusion |
Article Readings:

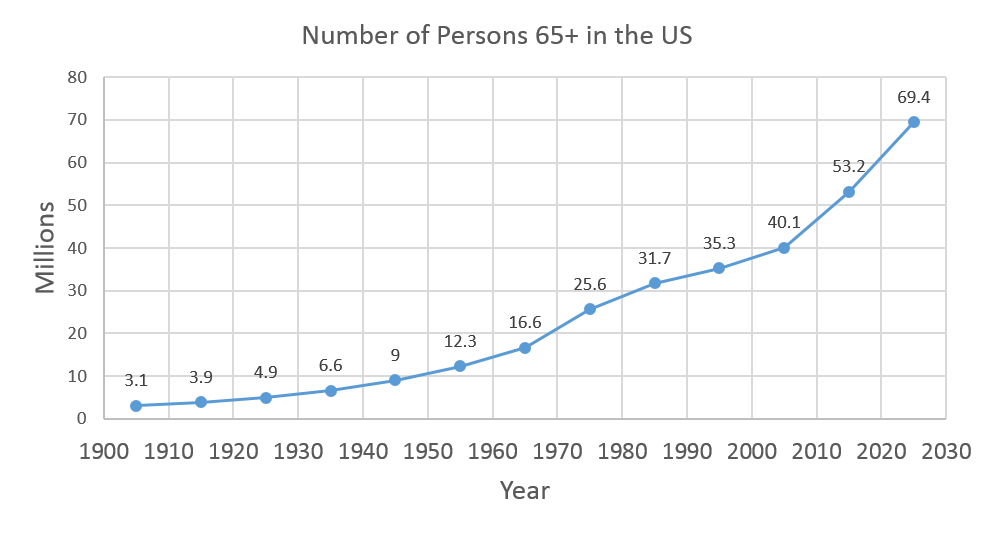
There are so many disciplines and specialties in medicine and health care—it can be overwhelming. The health care sector of the U.S. economy continues to grow due to population growth, with an emphasis on immigration into the country, and the graying of America, especially as the Post-World War II Baby Boomers (those born between 1946 and 1964) begin to reach retirement age.
See Figure 1 below for the growing numbers of older people in the US by decade. This indicates roughly the number of people who will be able to participate in certain government programs such as Medicare and Social Security. As you can see from the figure, this number has already increased dramatically over the last 50 years and will continue to increase rapidly in the first part of the next century.
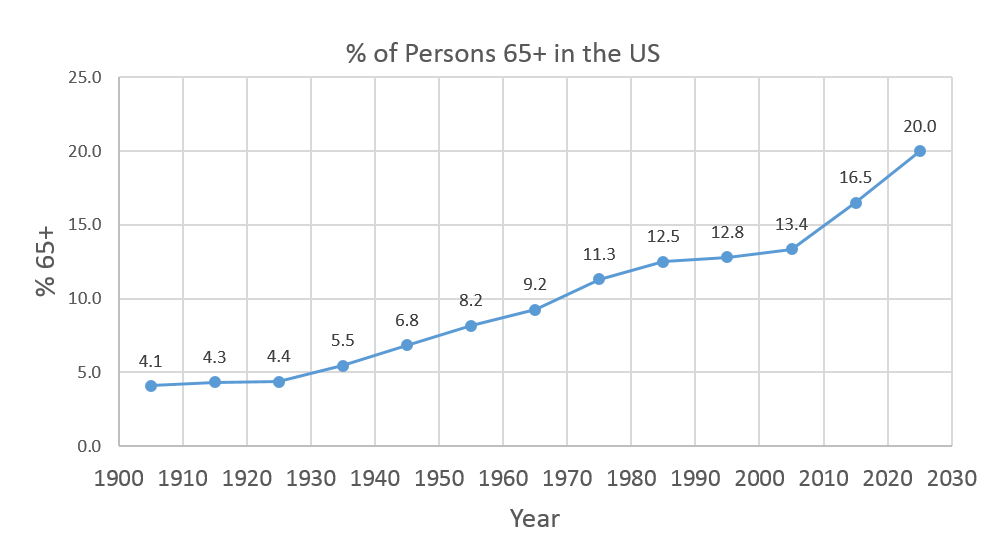
We have also seen growth in the percentage of the population that is older than 65. This also has been growing for about a hundred years. Note the sharp increase 2010 and 2020. Baby Boomers started to become Medicare eligible in the early 2010s.
|
|
|
How do students (younger and older) choose the careers they ultimately go into? What are the incentives? What are the rewards? Perhaps the incentives are the need to work with people, the need to contribute to the prevention and treatment of disease, or the need to change the world. For some, salary may also play a large role, especially if they are facing the possibility of $300,000 worth of debt following graduation.
In 2012 there were 13.5 million people employed in health care settings. Even with the recent recession and moderate unemployment rates across the country, the health care industry continues to add jobs. Of the 30 occupations projected to have largest percent increases in jobs between 2012 and 2022, 14 of those occupations are related to health care. Over this time the overall labor force is predicted to grow at 0.6% annually. In health care the predicted annual growth is 2.6%. This adds up to of 5 million jobs in a decade.
The University of Pennsylvania opened the first US medical school in 1765. The curriculum included intestinal purging and blood-letting. Many practicing physicians had not attended any formal educational program and were trained by apprenticeship. In the early 1800s the field of medical education evolved to include uniform academic preparation. Today a person becomes an MD (Doctor of Medicine) or a DO (Doctor of Osteopathy) by education. The degree is only the start of the process. The license to practice medicine comes from each state, there is no national system. In most states the scope of practice is the same for MDs and DOs.
Massachusetts policy defines the practice of medicine as follows:
|
"The Practice of Medicine means the following conduct, the purpose or reasonably foreseeable effect of which is to encourage the reliance of another person upon an individual's knowledge or skill in the maintenance of human health by the prevention, alleviation, or cure of disease, and involving or reasonably thought to involve an assumption of responsibility for the other person's physical or mental well being: diagnosis, treatment, use of instruments or other devices, or the prescribing, administering, dispensing or distributing of drugs for the relief of diseases or adverse physical or mental conditions. (a) A person who holds himself or herself out to the public as a physician or surgeon, or with the initials "M.D." or "D.O." in connection with his or her name, and who also assumes responsibility for another person's physical or mental well-being, is engaged in the practice of medicine." |
Minimum requirements for an initial license in Massachusetts include the following:
|
Physicians wishing to practice in additional states must make arrangements with the individual Board of Registrations. Scope of practice regulations for any licensed medical profession are state-based. There are additional guidelines for International Medical Graduates (IMG) to allow entry to practice without repeating the complete training.
Primary care physicians (PCPs) provide preventive services and treat frequently occurring and less severe problems, while specialists must have certification in an area of medical specialization. This requires additional years of advanced residency training followed by several years of practice in that specialty.
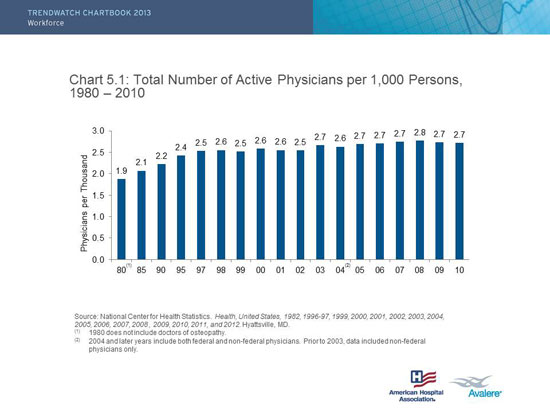
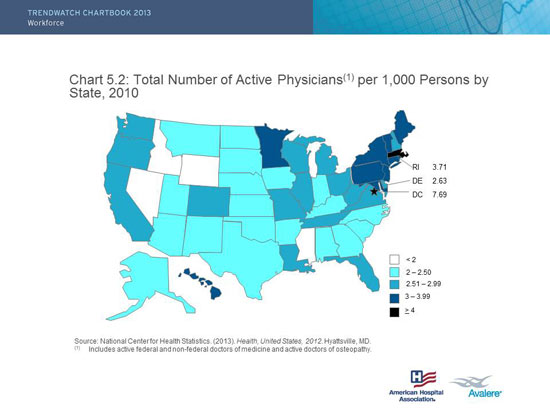
In addition to the sharp increase in the physician labor force in the US (resulting in a current oversupply), there also exists a "maldistribution" of physicians. Not only does the physician supply exceed previous projections (as well as future growth projections through the first decade of the 21st century), a surplus of physicians, among other issues we are discussing, can lead to increases in health care expenditures. This is an example of a geographic maldistribution. The number of MDs per 1000 persons is slightly increasing, or constant. The distribution across the United Stated is skewed. Note the data are adjusted for the state population.
There are two concerns. First, physician distribution across the United States is skewed (see figure). Second, it is believed that the US has far too many specialists and a shortage of primary care physicians. Specialty care is concerning because care is generally more resource incentive, tend to order more tests and procedures- resulting in higher cost. Furthermore specialists focus on their own specialty, and patient care can become fragmented without the holistic perspective of primary care to coordinate.
Explore the two statistical data graphs below from the report.
|
|
|
Source: AHA Chartbook: Trends Affecting Hospitals and Heatlh Systems
Many factors go into the decision of a physician to practice primary care including academic interest, availability of training opportunities, work-life balance, and potential income. The reality is that medical education is incredibly expensive. Specialists are paid more than primary care physician and so the ability to repay school loans is an important factor to consider.
Definition of a Hospitalist and Hospital Medicine
Hospital medicine: A medical specialty dedicated to the delivery of comprehensive medical care to hospitalized patients. Practitioners of hospital medicine include physicians ("hospitalists") and non-physician providers who engage in clinical care, teaching, research, or leadership in the field of general hospital medicine. In addition to their core expertise of managing the clinical problems of acutely ill, hospitalized patients, hospital medicine practitioners work to enhance the performance of hospitals and healthcare systems by:
Though the concept appeared a bit strange to many patients at the outset, and some patients still ask, "Where's my doctor?" hospitalists are often much more familiar with the hospital and its systems and functions. Because the hospital is the primary site of their practice, they are usually able to spend more time with patients than physicians who must juggle office patients, transportation, and often have to see their patients in between other commitments (early morning, at lunch, or at the end of a long day after office hours).
For the hospitalist model to work there must be processes in place to allow two-way communication between the hospitalist and the primary care team. Access to the patient's medical information is key. Once the patient is ready to be discharged the hospitalist must ensure there is a plan in place for a smooth transition to home and community medical services. The PCP needs access to records form the hospitalization to ensure continuity of care after discharge.
|
Employment Settings of Registered Nurses*
*Percents may not add to 100 due to the effect of rounding. Only RNs who pridived setting information are included in the calculations used for this figure.
|
Nurses and allied health professionals work in a variety of settings including, but not limited to: hospitals, nursing homes, private practices, ambulatory care centers, community, and migrant health centers, emergency medical centers, managed care organizations (MCOs), workplace settings, government and private agencies, clinics, schools and colleges, retirement communities, rehabilitation centers, as private-duty nurses in patients' homes, and as clinical researchers.
The career path for nurses is complicated by the fact that nurses are classified by both education (from a hospital school, college or university) and licensure (by individual states). There is increasing pressure from academic institutions and from accrediting organizations (Magnet) to make the BSN (Bachelor of Science in Nursing) the entry degree.
Source: AARP and RWJF, 2010.
APRN: Advanced Practice Registered Nurse
APRN: Advanced Practice Registered Nurse
SNF: Skilled Nursing Facilities
The lack of clarity on who is a nurse and how to become a nurse created problems in the workplace and in student recruitment efforts.
|
What are APRNs?
Types:
APRNs: Nurse Practitioners (NPs)
|
For this course, when I talk about nurses, I am referring to RNs, unless otherwise specified. When I refer to APRNs, I am grouping together the advanced practice nurses including nurse practitioners, nurse midwives, and nurse anesthetists.
The distinction between registered nurses and APRNs is especially important and this influences scope of practice. You can see above that over time the proportion of nurses with diploma training has decreased, replaced by greater proportions of nurses with associates or bachelors degrees. A Master's degree is now required for all APRNs, and there is talk of the Doctorate (DNP) becoming the entry to practice degree for NPs in the near future.
You may find this Nurse Licensure Map to be a useful summary.
Brought to you by Nursing License Map and Nursing@Georgetown.
Source: http://nursinglicensemap.com/pathways-in-nursing-infographic/
Consider this in terms of quality, cost and access.
Quality: Evidence that care by RNs is associated with patient outcomes
Many recent studies point to the connection between adequate levels of registered nurse staffing and safe patient care.
Cost: Evidence that care by RNs and APRNs is cost savings
Access: Evidence that increased use of RNs and NPs increases access to care
The nursing shortage can be examined from four different perspectives:
Increasing Demand
Decreasing Supply
|
US DHHS 2010 from National Sample of RNs
Source: bhpr.hrsa.gov/healthworkforce/.../rnsurveyinitial2008.pdf |
Challenges
Solutions
The figure below shows a health policy solution. Individual states have begun to propose legislation for staffing standards for inpatient care.
|
President Obama Addresses the Nursing Shortage Source: http://youtu.be/N2R6vRn0p9I |
Nurse Reinvestment Act of 2002
We started with physicians because then have the power. We concluded with nurses because they have the numbers. We have not done justice to the dozens of other health professionals working in hospitals, ambulatory care and community health. It is important to understand the roles of these other team members as a health care consumer, and for your own career development.
Now that we have briefly explored the world of medical doctors who work in various settings, here are a few other health professionals that are also integral members of the American health care team. Due to the great depth and volume of health care provider information that is beyond the scope of this course, only general information is provided here, with some helpful links for further exploration. These include dentists, pharmacists, other doctoral-level professionals, and a special section on nursing and the growing shortages that are facing this and other health care professions today.
Dentists are the major providers of dental care and must have graduated from accredited dental schools that award a Doctor of Dental Surgery (DDS) or Doctor of Dental Medicine (DMD) degree and successful completion of both written and practical examinations. Specialties recognized by the American Dental Association (ADA) include orthodontics, oral and maxillofacial surgery, oral pathology, pediatric dentistry, prosthodontics, periodontics, endodontics, and public health dentistry. For more information on this profession, go to the American Dental Association.
Pharmacists dispense medicines prescribed by physicians, dentists, and podiatrists and provide consultation on the proper selection and use of medicines. They too must have graduated from an accredited pharmacy program that awards a Bachelor of Pharmacy or Doctor of Pharmacy (PharmD) degree, successful completion of state board examinations, and practical experience or completion of a supervised internship.
The role of pharmacists has expanded from the preparation and dispensing of prescriptions to include:
(OD degree)—vision correction
American Optometric Association
(PhD) or (PsyD) degree—mental health counseling and psychotherapy
American Psychological Association
(DPM)—diseases and deformities of the feet
American Podiatric Medical Association
(DC)—the art of manipulation and joint mobilization, rooted in the belief that the health of the spinal column and nervous system is central to well-being.
American Chiropractic Association
(DPT)—See more information under the "Allied Health" segment
American Physical Therapy Association
(OTD)—See more information under the "Allied Health" segment
American Occupational Therapy Association
See more information under the "Allied Health" segment
American Speech-Language-Hearing Association
As seen above, many nurses, PTs, OTs, and SLPs also receive PhDs and professional doctorates today, though most can be certified to practice clinically with a Bachelor's or Master's degree.
One last shout out will be for Child Life Specialists. Before I became a nurse I had been a volunteer in hospital playrooms and taken related coursework.
Hospital Specialists Help Remind The Sickest Kids They're Still Kids
NPR, June 2012
After payment for hospitals, payment for providers (most of them physicians) is the largest health expenditure in the US. When you stop and think about it, physicians make the decisions which drive the cost for most of the system (treatments, tests).
How physicians are paid makes a difference. Each method of payment has a purpose or intended consequence. Methods of payment also create financial incentives, and some of these incentives may have negative effects on access, quality, and cost. Look at the table below. For each method of payment you have been given the intended consequence and an example. Your task is to match each method of payment to a potential negative affect.
|
Intention |
Unintended Consequences |
Example |
|
|
Fee for Service |
Compensates providers according to efforts and resources used |
Increases unnecessary treatments and procedurees to increase volume |
Traditional Medicare (Part B) pays providers using RBRVS |
|
Per Illness Episode |
One fee covers procedures and follow up visits; decreases unnecessary visits |
Provider minimizes post-procedure visits |
Surgeons payment is for the procedure and post-operative care |
|
Capitation |
Allows provider to direct resources toward mazimizing patient health |
Providers may skimp on care maximize their profits |
Medicare Part C plans (Medicare Advantage) |
|
Salary |
Remove financial incentives for over and under treatment |
No incentive to work hard or more efficiently or to be cost-donscious |
Veterans Health Administration |
|
Pay for Performance (P4P) |
Bonus for meeting quality or efficiency benchmarks established by payor OR assign a penalty for failing to meet benchmarks. Aligns provider goals with those of the payor. |
Providers concentrate on benchmarks to the exclusion of other important care elements. May also penalize providers with many complex apatients. |
ACO shared savings bonuses for primary care performance from ACA |
AMA Mission & Guiding Principles
Mission: To promote the art and science of medicine and the betterment of public health.
Our guiding principles set the aspirations that we endeavor to achieve:
From www.ama-assn.org/ama/pub/about-ama/our-mission.page
The AMA is a large and powerful physician organization. The leverage of the AMA and state medical associations far surpasses the ability of individual physicians to influence practice and policy. Historically the AMA has protected the interests of physicians and often lobbied against health insurance, expansion of scope of practice for non-MD practitioners, and health reform. The AMA is certainly not the only influential health care lobbying group, but they are one of the more influential. Other players include associations of hospitals, associations of insurance groups and the pharmaceutical industry. The non-governmental organizations involved with education, lobbying and research three different types:
Lobbying On Health Care Issues Falls In 2010

Source:: www.kaiserhealthnews.org/Stories/2011/January/27/health-care-lobbying-spending-chart.aspx
Physicians have an exclusive scope of practice based on training and expertise. State laws uphold the rights of physicians to stake claim over areas of clinical practice. There are challenges, or turf wars, between groups of MDs and between MDs and non-MD providers. On the surface these battles may center on competency, quality, and safety. There is usually an underlying aspect of finance and protecting one's revenue source. If a group has exclusive rights to perform procedure X that group is not going to welcome other provider types into that market. The group often brings up concerns about quality. When there are also concerns about money, or turf protection, those are not made explicit.
The national shortage of primary care MDs is expected to worsen as health care reform expands access to currently uninsured Americans. One logical solution would be to extend the scope of practice for nurse practitioners (NPs) to allow for more independent practice.
Expanding scope of practice for NPs often creates pushback from associations on the national and local level for physicians. The goal of an interest group for physicians (or any other profession) is to protect the financial interests of its members. If NPs are able to provide more care independently this could threaten physician market share.
There are countless examples of this behavior across the medical professions. Several are bound to pop up on Kaiser Health News over the course of the semester. The specifics differ by state as scope of practice and licensing rules are under state jurisdiction.
They are all variations of the same theme:
Here are some examples:
In Massachusetts Certified Nurse Midwives had an expansion of scope of practice allowing them to work more independently and to partner with family practice MDs (previously had to be with OB/GYNs). The Massachusetts Medical Society testified against the bill. The bill passed.
A second bill was proposed related to Professional Midwives or Lay Midwives. The Massachusetts Medical Society protested. Local associations for nurse midwives (Certified Nurse-Midwife or CNM) were also against the legislation. The bill did not make any progress.
|
Source: http://youtu.be/CE48gVSWygk |
We will start with trends in hospital utilization and the role of the hospital as an employer using data from the American Hospital Association.
|
|
Total Number of All US Registered Hospitals |
5,753 |
|
Number of US Community Hospitals |
4,999 |
|
Nongovernment Not-for-Profit |
2,849 |
|
Investor-Owned (For-Profit) |
1,068 |
|
State and Local Government |
1,037 |
|
Federal Government Hospitals |
211 |
|
Nonfederal Psychiatric Hospitals |
413 |
|
Nonfederal Long Term Care Hospitals |
89 |
|
Number of Hospital Units of Institutions |
11 |
| Source: AHA Fast Facts 2014 | |
When people think about medical care they often think about hospitals. Over time more services have moved out of the hospitals into day surgical centers, ambulatory care, rehabilitation centers, and community-based programs.