Another useful way to weigh benefits and risks is to compare risk differences.
This gives a useful perspective on the actual numbers of people who might
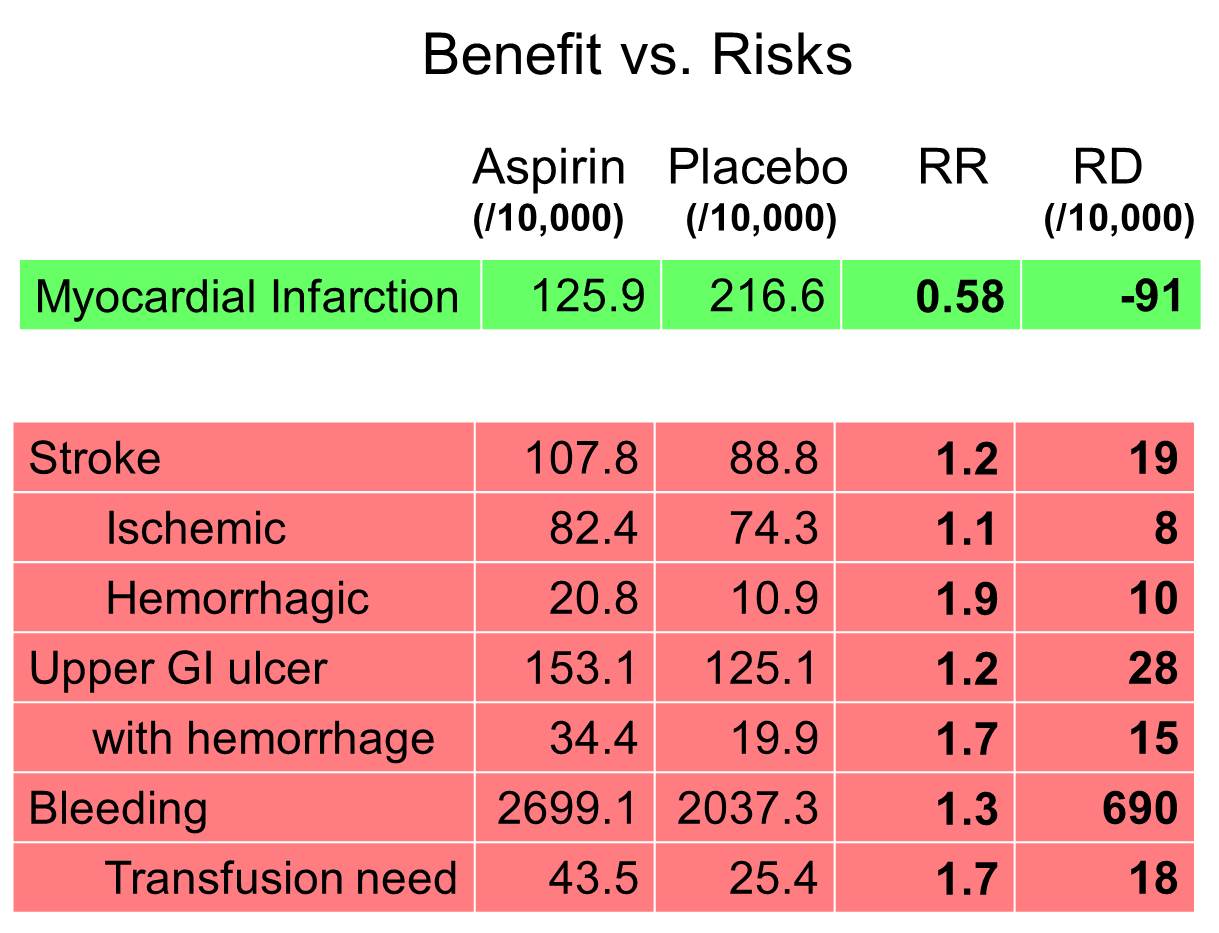
benefit or be placed at risk by a treatment. The table below looks at the same
data that was presented in the previous table, but from the perspective of risk
difference, rather than risk ratios.
This table would suggest that for every 10,000 men treated with low dose aspirin there are 91 fewer myocardial infarctions, but this benefit must be balanced against 10 more hemorrhagic strokes, 28 more upper GI ulcers and 18 more bleeding problems requiring transfusion. A balance sheet like this informs the discussion between an individual patient and their physician and promotes "informed" decisions about therapy.
A similar approach was used in a recent analysis in which the authors conducted
a risk-benefit analysis for celecoxib versus low dose aspirin in patients with
colonic adenomas. The authors concluded that two clinical trials provided strong
evidence that, among patients with colonic adenomas, the use of celecoxib
reduced metachronous adenomas, but the trials were too small to evaluate their
role in preventing cancer. Nevertheless, there was a significant risk of
cardiovascular side effects, and even if one used optimistic estimates of the
ability to prevent colorectal cancers, the increased risk of cardiovascular
events outweighed the potential benefits with respect to cancer prevention.
Psaty BM and Potter JD:
Risks and benefits of celecoxib to prevent recurrent
adenomas. (N. Engl. J. Med. 2006;355(9): 950-952.)