

Overview
Lyme disease is a vector-borne disease caused by transmission of bacteria through a tick bite. Lyme disease is caused by a gram-negative bacterium of the spirochete phylum called Borrelia burgdorferi (see photo to the left below). If a tick bite deposits a sufficient number of the bacteria into a human host's skin, the bacteria replicate in the dermis layer of the host's skin at the site of the tick bite, often causing the appearance of a characteristic "bull's eye rash," also known as erythema migrans (see photo to the right below). If it is not treated promptly, the bacteria can spread to the bloodstream and infect the joints, heart, and central nervous system causing a variety of symptoms and manifestations.
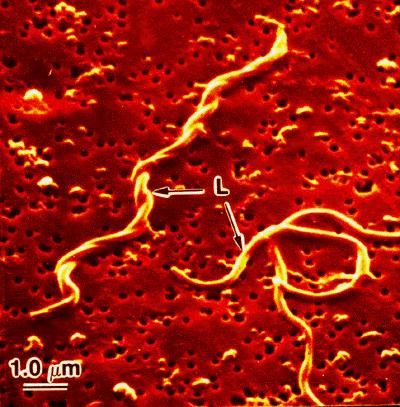
Borrelia burgdorferi
Source: http://borrelia.mlst.net/

Erythema migrans or "bull's eye rash")
Source: http://hardinmd.lib.uiowa.edu/CDC/lymedisease7.html
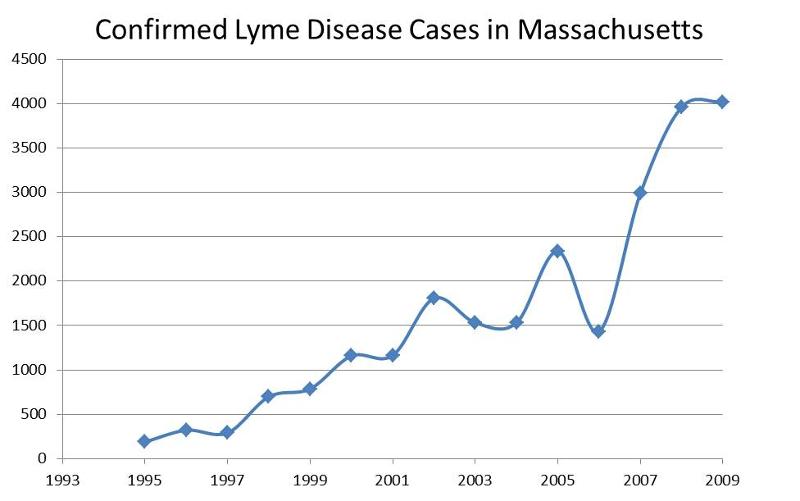
Magnitude of the Problem
In 2009 there were 29,959 confirmed and 8,509 probable cases of Lyme disease reported to CDC, for an incidence of 13.4 cases per 100,000 population. During the same year, Massachusetts had 4,019 confirmed and 1,237 probable cases, an incidence of 61.0 per 100,000 population. The annual number of confirmed cases has been rising steadily over the past 15 years.
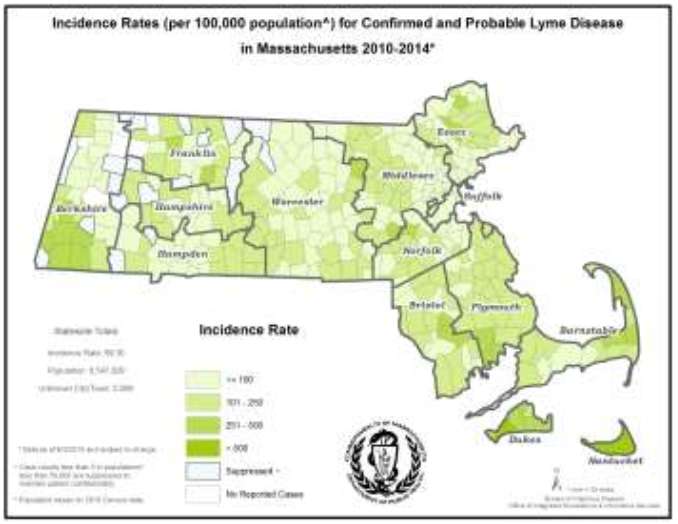
Geographic Occurrence
The incidence of LD is associated with the density of infected tick vectors. Most cases in the U.S. have been reported in the Northeast, the western states, and the upper Midwest, but nearly all states have reported Lyme disease. The US map below is from CDC and based on 2009 data. The Massachusetts map shows Lyme disease incidence rates per 100,000 by town in 2005. Darker shading indicates higher incidence. Lyme disease is considered endemic in the entire state of Massachusetts. Areas of highest incidence include Cape Cod and southeastern Massachusetts, the islands of Nantucket and Martha's Vineyard, areas north of Boston in Essex county, towns along the upper Middlesex and Worcester county border, along the Quabbin Reservoir watershed, and in southern Berkshire county.
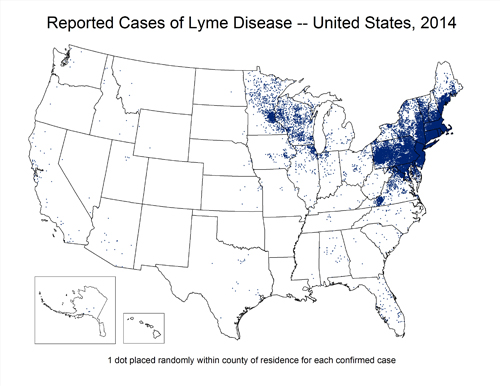
Source: http://www.cdc.gov/lyme/stats/maps.html
Source: http://www.westfordma.gov/pages/government/towndepartments/westfordma_healthcare/tick
Table - 2013 Confirmed and Probable Cases of Lyme Disease by County
|
County |
2013 Confirmed Cases |
2013 Probable Cases |
Incidence of Confirmed + Probable per 100,000 |
|---|---|---|---|
|
Barnstable |
186 |
88 |
127 |
|
Berkshire |
84 |
46 |
99 |
|
Bristol |
413 |
162 |
105 |
|
Dukes |
32 |
38 |
423 |
|
Essex |
405 |
154 |
75 |
|
Franklin |
51 |
20 |
100 |
|
Hampden |
167 |
57 |
48 |
|
Hampshire |
112 |
35 |
93 |
|
Middlesex |
720 |
267 |
66 |
|
Nantucket |
47 |
16 |
619 |
|
Norfolk |
460 |
150 |
91 |
|
Plymouth |
631 |
231 |
175 |
|
Suffolk |
81 |
49 |
18 |
|
Worcester |
480 |
194 |
84 |
|
Unknown |
211 |
76 |
- |
|
State Total |
4,080 |
1,585 |
65.1 |
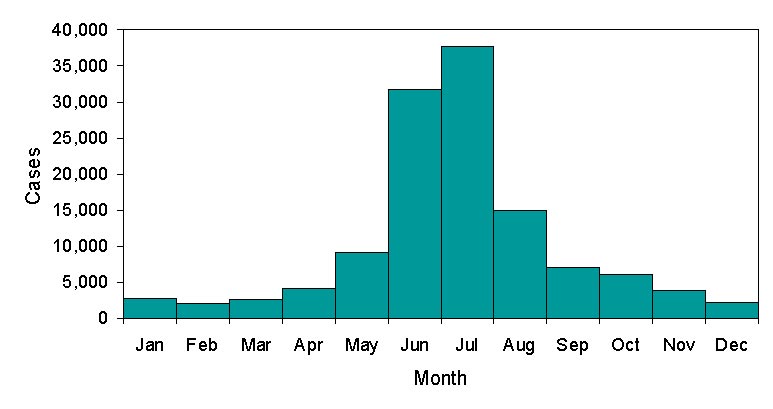
Seasonal Occurrence
In Massachusetts, the highest risk of exposure to nymphs occurs during the spring and early summer, and the highest risk of exposure to adult ticks occurs during later summer into fall. Most cases have their onset between April and October, when the risk of contact with infected nymphal ticks is greatest. The graph below is from CDC.

 |
Reporting Cases of Lyme Disease Click below the question to view the answer. |
|
This content requires JavaScript enabled.
|
|
Surveillance for Lyme Disease
Unlike most reportable diseases in Massachusetts which rely on follow-up of laboratory case reports by the local Board of Health, Lyme disease utilizes a physician-based reporting system. The Massachusetts Department of Public Health receives notification about most suspect cases of Lyme disease through receipt of positive laboratory tests which are submitted directly to the DPH Integrated Surveillance and Informatics System (ISIS) by laboratories. Receipt of a positive laboratory report generates a letter from ISIS to the physician with a teleform case report form for them to provide clinical information on. Local Boards of Health receive notification of positive laboratory results about residents as well but are not required to follow-up although they may choose to do so. Boards of Health that are trained on MAVEN are notified through that route; Boards of Health not on MAVEN receive a linelist of reports monthly.
Physicians are legally required to submit clinical information on any case of Lyme disease that they diagnose although this is an unreliable reporting method due to the heavy burden it places upon healthcare providers. However, some of the notification DPH receives about cases does originate from physicians reporting cases they have seen.
After clinical information is received by ISIS, the completed case report is reviewed by an epidemiologist at DPH and the standardized, national case definition is applied. The case definition separates cases into confirmed, probable and suspect cases based on consensus guidelines developed by the State Epidemiologists from all 50 states. The case definition can be viewed at: http://www.cdc.gov/osels/ph_surveillance/nndss/phs/infdis2011.htm. A large proportion of Massachusetts cases fall into the suspect disease category simply because DPH never receives any clinical information regarding a patient with a positive laboratory test. Because laboratory testing alone is not sufficient to identify cases of disease, these cases cannot be included in Massachusetts case counts of confirmed and probable cases which are the numbers that are reported to CDC and available for public release.
The local Board of Health also receives notification of the positive lab reports but is not expected to do any case investigation.
Note that there is controversy regarding reporting of Lyme disease discovered in its later stages. The CDC case definition is restricted to early cases of Lyme disease, while Massachusetts uses a broader definition that includes both early and late states.
lLink to a discussion of the controversy.